Surgery Fundamentals: Waiting Lists, Processes & More - Academy
Blog Post

In this blog
- Hospital Waitlist Basics
- How Surgery Waitlists Work
- Why We Need Surgery Waitlists
- Challenges with Surgery Management and Wait Times
- Strategies for Managing Surgical Waitlists
- Manage Surgical Waitlists with Hospital Improvement Software
- Start Improving Surgical Waitlists Today
- Learn More: Resources for Surgery Management
- Share Your Knowledge

Whether you’re a surgeon, scheduled care manager, theatre manager, or hospital administrator, managing (and possibly improving) the elective surgery waitlist is a fundamental part of overall hospital operations.
But long wait times for elective surgery (where patients wait longer than clinically recommended timeframes) are a near universal problem, impacting public hospitals everywhere.
| Managing (and improving) your elective surgery waitlists is a fundamental part of overall hospital improvement. |
So, why are surgical waitlists so hard to manage? And what can we do about it?
Long waits for elective surgery are a complex problem, driven by a number of factors. So, let’s break it down to understand what might be causing your overdue patients — and some of the strategies you can use to start fixing the problem.
We’ll look at surgical waitlist management from nearly every possible angle, from why it’s so challenging to get right (and especially why right now), and what steps you can take to better understand and manage your surgical waitlists. Plus, some useful resources you can explore further and apply to your own specific challenges within your surgery department.
| Note: We’re talking specifically about waitlists and the duration of time patients are waiting for their elective surgery (which could be days, weeks, months, or years). We’re not referring to the time spent sitting in the admissions unit on the actual day of surgery. |
You may find waitlists at three points in the patient journey:
1. Outpatients
After a patient is referred to a hospital specialist, they’ll go on a waitlist for an outpatient appointment.
Learn more about outpatient waitlist management here.
2. Medical Imaging
If a patient requires imaging to assist with a diagnosis or to plan a procedure, they may go onto a waitlist for a CT or MRI.
3. Elective surgery
After attending an outpatient appointment, if a patient needs surgery, they may be added to an elective surgery or procedural waiting list. This can happen after the first outpatient appointment if their condition is clear. Or it may be after their clinician confirms a diagnosis and determines their treatment plan during a review appointment.
Before putting someone onto a waitlist, medical staff review the patient’s condition to categorise it based on urgency. This ensures that the system is enabling those that have the greatest clinical urgency to be seen first.
These categories often come with time-based guidelines to ensure that patients are seen within a clinically recommended timeframe. For example:
- Urgent – 30 days
- Semi-urgent – 90 days
- Routine – 1 year
Categories vary between different hospital systems, along with the clinically recommended timeframes. But the idea behind them is universal. Patients should gradually move up the queue and be seen by a surgeon in the order that they joined the waitlist.
Unfortunately, not all patients receive treatment within the clinically recommended time. For example, take a look at the following hip replacement surgery treatment times.
| Hip Replacement Surgery Waitlist Data A report from OECD shows that in 2018, the median wait time for hip replacement surgery (averaged across 12 countries) was 113 days. This included Australia (119 days), Canada (105 days), United Kingdom (95 days), and New Zealand (81 days). To get an idea of where this figure is likely to sit now, in 2020-21, 20.6% hip replacement surgeries in Australia had waited more than 365 days for treatment, compared to 5.6% in 2018-2019. |
Check out this surgery waitlist data to understand more about what wait times currently look like in public hospitals around the world.
Surgical waitlists are useful for public hospitals for three main reasons.
1. To Balance Demand & Capacity
Quite simply, surgery waitlists help manage demand and capacity. A waitlist is a tool to help you understand the incoming demand so you can allocate appropriate resources to meet patients’ needs.
If patients on the waiting list are within their clinically recommended timeframe, it can be an indicator that demand and capacity are in balance (it may also mean capacity is higher than demand, though this is very rare).
However, if patients on the waiting list are waiting longer than clinically recommended timeframes, it can be a sign of one or more of the following:
- Demand exceeds available capacity to treat the patients
- Capacity is not distributed to meet the demand and may need to be reallocated or substituted
- There are operational processes (like bookings) that are causing patients to wait too long to be seen
This is why surgery wait times are an important performance metric (perhaps one of the most important metrics) for hospital management, health departments, heads of units, clinicians, and booking officers.
| A waitlist is a tool to help you understand the incoming demand so you can allocate appropriate resources to meet patients’ needs. |
A tool to assist with managing demand isn’t unique to hospitals. Waitlists or queuing systems are seen in nearly every business where demand exceeds the capacity available to deliver goods or services.
For example, if you go into your local coffee shop at peak hour and there’s only one barista manning a single machine, you wouldn’t expect to skip to the front of the queue. They might have five people in front of you to serve first, and 10+ beverages to make. If you really want that coffee, you’ll join the queue and wait your turn, like everyone else.
But of course, there’s a lot more at stake than caffeine headaches when it comes to hospital waitlists. And figuring out who gets served next isn’t quite as simple as saying ‘next please’.
2. To Ensure Equity
Embedded into best practice waitlist management is the concept of ‘equity’. It’s not fair if you have to wait years and years because you can not afford private healthcare. Public health should provide an equitable service to the community, regardless of financial circumstances where they are located. This is important because public healthcare is funded by federal and state governments using funds raised from taxes.
| Good waitlist management will ensure that the system is equitable for everyone. |
Good waitlist management will ensure that the system is fair to everyone on the waitlist — and that people who can’t afford private health do not wait longer than clinically recommended times (and then receive poor health outcomes).
3. To Improve Health Outcomes
A patient that isn’t seen in time could experience worse health outcomes that have a big impact on their quality of life, their livelihood, and their relationships. While waiting for surgery, their condition could deteriorate and cause other problems throughout their body and/or lead to more complex surgeries and longer recovery times.
For example, consider a patient who is waiting for cataract surgery. If that patient waits too long, their eye sight could deteriorate and they could temporarily lose their driver's licence. This could mean losing their access to the community, depending on community support for transport, and greater social isolation. They are also more likely to fall within their home environment because they can’t see well enough to respond to environmental obstacles. Falling could lead to new health issues such as wrist, rib and hip fractures — plus the need for home modifications and walking aids in future.
When managed properly, waitlists should support patients to be seen in time, leading to better health outcomes (and minimising added complications).
Read more about the impact of improving surgical wait times.
Why is it so tricky to manage surgical waitlists?
We’ve already discussed how waitlists exist as a management tool for hospitals to understand demand. The reason it’s so tricky to manage surgical waitlists is because there are a lot of factors that influence demand — and a hospital’s ability to respond to that demand. As a result, we get demand and capacity imbalances that lead to longer waiting times for treatment.
So, let’s unpack some of the demand and capacity challenges facing hospitals right now.
Unplanned Surgery
When managing elective surgery, you can have the best scheduling processes in the world, but you’ll always have to prioritise emergency cases.
| Elective surgery is done on any patient that has been referred for surgery or entered the system through a planned care pathway. Emergency surgery includes any procedure that was unexpected or unplanned. Most people requiring emergency surgery come in via the emergency department. |
Emergency cases are patients who require unplanned surgery. Unlike elective surgery patients who are referred by a GP and seen in outpatients first, these patients usually present to hospital first via the emergency department. Their need for treatment is triggered by one of three things:
- Trauma – For example, a fall, car accident, or workplace injury
- New and acute condition – For example, appendicitis
- Chronic condition deterioration – Their pre-existing chronic condition (e.g. diverticulitis) has rapidly deteriorated
If your allocated resources for emergency surgery aren’t sufficient at any given moment, you’ll need to pull additional resources away from planned surgeries. This can require hospitals to reallocate theatres, surgeons, and beds, leading to delays and reschedules for planned surgeries. In turn, having an impact on surgery waitlists.
Limited Beds
If a bed isn’t available, surgery can’t go ahead — in some cases, this includes both inpatient beds and ICU beds. In public hospitals, this is quite common because they operate at near full capacity. Even with the best planning and strategies such as ‘elective surgery bed caps’, hospitals still frequently experience bed shortages for elective patients.
Some of the most common reasons hospitals end up short on beds include:
- Unexpected complications – Patients who are booked for a ‘day case’ sometimes experience a routine (but unexpected) complication that requires overnight observation, tying up a bed that was originally allocated to a planned overnight case
- Slower than expected recovery – Sometimes patients occupy a bed for longer as they haven’t recovered as quickly as expected, which reduces bed availability for new planned cases
- Surge in ED cases – While emergency cases wait on the emergency board, they may require an admission for observations/care
- Unplanned maintenance – Rarely, a bed, room or ward may require unplanned maintenance, making the space unavailable for use (when this happens, elective surgery is often affected first, as it’s easier to cancel patients than redirect emergency admissions to another hospital)
- Waiting on imaging for discharge – If there are backlogs in imaging preventing discharge, patients may occupy a bed longer while waiting for an MRI or EEG
- Surge in admissions – If there’s a surge in medical patients requiring admission (e.g. COVID-19 cases), these may occupy beds that would have otherwise been used for elective surgery
Limited Theatre Availability
If a theatre isn’t available, the surgical procedure can not go ahead and some patients will need to be rebooked. Some reasons this might happen include:
- Booking errors – Patients were booked onto a list that did not have a theatre assigned
- A surge in emergency surgeries – Theatres and resources are reallocated to manage more urgent cases
- Unexpected maintenance – Issues such as a lighting or equipment failure can mean that the theatre is not able to be used until repaired
- Planned surgeries running overtime – If a surgery takes longer than expected, patients scheduled for the end of the list are more likely to be cancelled than those at the start
Limited Specialists
If a surgeon isn’t available, the surgical procedure can not go ahead. Because there are limited numbers of specialised clinicians who are trained, qualified, and authorised to admit and operate at each hospital, any disruption to their availability can impact waitlists. As specialist consultants become even more specialised — for example, Orthopaedic Surgeons can be lower limb, upper limb, hand, foot and ankle, or spinal specialists — this becomes even more pertinent.
Smaller speciality teams, such as vascular and neurosurgery, are often more subject to cancellations due to emergency cases, as well. This is because less staff are available to complete the emergency case — and if it occurs overnight, the surgeon on call must attend and is then unavailable to complete their list during the day (due to fatigue management). Even if the emergency case can be stabilised until the morning, it’s likely that the surgeon allocated to the patient already has an elective list planned for that day. And if they have a fully booked list, it is likely that some (if not all) cases will end up being cancelled.
The Theatre Schedule
Managing theatre schedules is a challenge in itself that tends to have a flow-on effect on surgery management and waitlists.
Usually a Nurse Manager is in charge of assigning the available theatre lists to specialties. And then the specialties assign this time to the surgeons. Unfortunately, theatre capacity doesn't always match up with the specialties that need it most. There's a number of reasons for this, like:
- Reliance on paper or excel spreadsheets, making it difficult to analyse demand and capacity and make informed decisions
- Waitlists focus on the number of patients, but provide limited visibility into theatre time required to treat those patients
- The use of quarterly master theatre schedules can lead to over-allocating sessions to some specialties, making it harder to fill these sessions closer to the time
- Some consultants have more influence than others, enabling them to secure theatre sessions that may not required
Learn more in our article on theatre schedule management challenges & strategies.
Lack of Staff
A lack of available staff, including surgeons, nursing staff, anaesthetists, and support staff could result in scheduled surgeries being cancelled. This could be due to holiday leave, sick leave, or even roster gaps and shortages.
Patient Cancellations
Patient-initiated day-of-surgery cancellations can disrupt schedules and theatre utilisation, as it’s often too late to book someone else.
Day of surgery cancellations can be unavoidable — for example, the patient developed a fever on the day of surgery. Or they can be avoidable — for example, they haven’t fasted, could not be located, or simply doesn’t show up for their admission on time.
Funding Sources — Blending Private & Public Healthcare
While approaches to funding differ between hospital systems, it’s common to see multiple revenue streams being used to resource their service model.
Some hospitals and jurisdictions look at ways to increase private funding through admitting both public and private patients. This practice can benefit both hospitals and doctors, as they’re not limited by state or health department budgets and billing constraints. It is also a great solution for regional hospitals to implement when they need to recruit new care providers to the area, as it offers an attractive incentive for specialised clinicians. However, one study suggests that this may play a role in increasing public patient wait times, as private patients may be given priority of access. So while this might resolve one problem, it may not benefit patients waiting for treatment on the public waiting list.
Population Changes
Many hospitals are positioned in growing populations, as well as ageing populations with growing health needs. But in healthcare, organisations tend to operate at almost full capacity almost everywhere — limited funding means there’s rarely resources allocated for future needs and growth.
| More people means more demand for elective surgery — but not necessarily the resources to meet this demand. |
Hospital strategy departments and divisions with Departments of Health invest a lot of time and money into modelling future needs. However the saying “what got us to here is not what will get us to there” is very pertinent in healthcare due to the advancements in diagnostic equipment and surgical procedures, as well as the development of disease modifying medications. As a result, it’s very rare for demand forecasts and bed requirement projections to have been accurate. They nearly always fall too far short or the beds are required far sooner than expected.
For example, Gold Coast University Hospital opened in 2013, with the expectation that it had enough capacity to meet local popular demand for 25 years. However, the hospital was full with all services activated by 2018 — around 5 years earlier than anticipated. Queensland Health is now planning a new hospital at Coomera (northern Gold Coast) to alleviate demand when it opens in 2028.
Incorrect Data
Too often, health services misunderstand and undervalue the impact that data management can have on patients and patient care.
For example, long waits (at least, to some degree) can occur because of the way some jurisdictions track and report on their waitlists. A lot of the time, only unbooked waitlists are reported on. But that doesn’t give the full picture — to understand and plan for total demand, you need to look at all the people on waitlists who are waiting for surgery (booked and unbooked). Not only that, but patients can become unbooked for a number of reasons, so it’s important to keep an eye on everyone until they receive care.
COVID-19
Last but certainly not least…
Surgical waitlist management has always required intentional management in order to reach the delicate balance between demand and capacity. The COVID-19 pandemic has had a significant impact on this balance, wreaking havoc on waitlists everywhere. The pandemic has caused:
- Hospitals to postpone elective surgery during COVID peaks
- Surgery waitlists to grow
- Some people to experience additional health challenges due to COVID delaying their surgery
- Substantial impacts on capacity due to ongoing staffing challenges
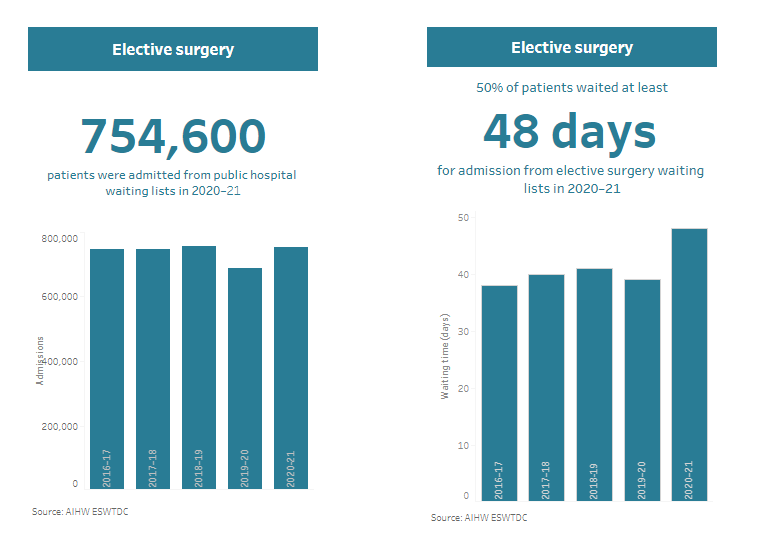
In Australia, for example, temporary restrictions were applied to some elective surgeries from March 26, 2020, resulting in:
- An overall surgery waitlist increase of 9.2% between 2018-19 and 2019-20
- 50% of 2020-21 elective surgery admissions occurring within 48 days, up from 39 days the previous year
- 7.6% of patients waiting more than 365 days for elective surgery in 2020-21, up from 2.8% the previous year
Further restrictions were applied throughout 2020-2022, varying by state. Similar measures have been applied in other regions, too. The flow-on effects will likely continue for some time.
Now healthcare teams must find a way to make up for lost time so that they can get waitlists back under control and treat patients within clinically acceptable timelines.
At the same time, COVID presents a unique opportunity to transform the way hospitals do things, including managing surgical waitlists.
As many surgical long waits are due to demand and capacity imbalances, all you need to do is reduce demand and increase capacity. Right? If only it were that simple…
| Because there are so many moving parts or ‘levers’ that interact and impact on surgical waitlists, it’ll take a team effort and strategies at every level in order to make a real change. |
Because there are so many moving parts or ‘levers’ that interact and impact on surgical waitlists, it’ll take a team effort and strategies at every level in order to make a real change.
So, we’ve assembled some of the top strategies and trends that are being used to tackle surgery waitlists in hospitals around the world.
Understand and Measure Your Progress
There is an expression that we very much believe is true…
| You can’t improve something you can’t measure. |
Apply this saying to waitlists and you get something like…
| Before you can do anything about your long waits or overdue patients, you first need to understand your numbers. |
The first strategy every hospital should explore is better data collection and analysis. You can use a platform like SystemView to:
- Know how many people are waiting for their procedure, if they are booked or not, and if they are overdue or not
- Understand how many people are coming onto and off your waiting list every week, and if you are ‘net’ in balance
- View how much theatre time you have access to, and how much of this is available
- Set a goal, know how many patients you need to be treating (or removing) each week to achieve this goal
- Monitor demand against capacity
When you’re faced with a big problem, it’s a good idea to break it into smaller, easier to solve parts. To apply this to your surgery waitlists, you can look at:
Specialties with the largest volume of overdue patients — To understand which specialities need intervention, and which do not
The category with the most longest waits — To understand the potential clinical risk and urgency
The patients waiting longest past their clinically recommended time — To address those that have been waiting the longest first
Combined, these will identify any performance and clinical risks that you need to tackle first.
Identify Trends and Plan Ahead
Demand for elective surgery is mainly driven by external factors — things that hospitals themselves can do little about. But hospitals can monitor that demand (i.e. the number of people going onto waitlists for planned surgery and those requiring unplanned surgery) to identify any trends and better plan for demand.
This can include planning for things like holidays and seasonal differences that may impact scheduling due to increased emergency presentations, staff holidays, and flu season cancellations. Not to mention factors like theatre closures and slow downs, surgical inpatient ward closures, and an inevitable increase in long waits for surgery.
Invest In a Theatre Operating System That Has An Electronic Theatre Schedule
Digital transformation projects are very common across healthcare at the moment, with more and more hospitals introducing electronic medical records and modern operating systems. One system that offers significant benefits is the Electronic Operating Theatre Schedule.
In the past (although this is still quite prevalent today), operating theatre schedules were created and stored in Excel spreadsheets. Excel is great because it is a very familiar tool for most users — and it tends to work well when there is a perception that not too many people need to see and or edit the schedule.
However, as hospital demand increases and clinical teams are held accountable for managing their own performance, a spreadsheet-based schedule becomes limiting. Teams are unable to see what they have coming up and they can’t easily access the information they need in order to inform their delivery plans.
On the other hand, an Electronic Theatre Schedule can display the number of theatres, the number and duration of lists (both open and closed), and the specialty and doctor allocated. This quickly becomes an important operational tool for health services because it enables powerful insights into the available capacity, which supports teams to get their demand and capacity in balance.
Use Guidelines, Clinical Standard Protocols, and Policies
Some clinical criteria for categorising patients isn’t well defined, like the appropriateness of surgical procedures or how likely the patient is to deteriorate. This means that to some degree, prioritising patient referrals is left up to the interpretation of individual surgeons and triaging teams.
Using a standardised tool with evidence-based criteria not only eliminates guesswork but makes accessing surgery more fair. Here are some examples of this in practice:
- Elective Surgery Services Implementation Standard (Queensland Health)
- National definitions for elective surgery urgency categories (AIHW)
- National Elective Surgery Urgency Categorisation (AHMAC)
Balance Outpatient & Surgery Flow
Before a patient goes on the elective surgery list, they first need an outpatient appointment to determine a suitable treatment plan. And before that, depending on the health service, they may need to go on the outpatient waitlist for their initial appointment.
This means that reducing long waits for outpatients (while a very good thing) will have consequences for surgical waitlists. You need to ensure balance across both departments by implementing measures to cope with the additional flow of patients to surgery.
Inside SystemView, you can use the Outpatients > Clinic Effectiveness > Conversions to Elective Surgery component to see your normal conversion rate from outpatient appointments to surgeries to understand how an increase in outpatient capacity might impact surgery waitlists, at a specialty and doctor level.
Audit Waitlists
It’s worth regularly auditing surgical waitlists, as this ensures a more accurate and up-to-date picture of demand. An audit involves contacting everyone on the waitlist (focusing on those that have been there the longest) to confirm their status. You can check whether their condition has improved or declined, if they’re still receiving the procedure, if they booked surgery elsewhere, or if they need to delay their surgical intervention. You may be able to remove some patients from the waitlist, and organise a treatment plan review for others.
Prioritise By Wait Groups
It’s much easier to organise your surgical waitlists if you can first sort your patients into groups.
In SystemView, for example, you can automate sorting patients into groups, like unbooked long wait, unbooked risk, unbooked, booked long wait, booked risk, booked in time, and booked to breach.
Each of these groups has different criteria and requires different actions to ensure they are booked in the right order, and that you minimise clinical and performance risk.
SystemView can provide Bookings Officers with a daily action list based on groups, showing which bookings to make next in order to reduce or avoid long waits for elective surgery. Plus, a list of patients to keep an eye on to ensure they don't get cancelled.
Read more about how using wait groups can help you organise hospital waitlists.
Create a Patient Tracking List (PTL) To Manage Overdues
One of the most straightforward but effective solutions to reducing surgery waitlists is to create a PTL that focuses on creating action plans for overdue patients. This allows you to focus on this patient cohort, so you can understand what actions and resources are required to treat (or remove) these patients and reduce the number of people who are overdue.
This strategy tends to be more effective if you can also book some patients that are within their target treatment times (to prevent other people from becoming overdue). But doing both at once is resource intensive and not always an option. That said, even if you don’t have additional resources, adopting a PTL approach or using wait groups to manage bookings will always help you minimise the number of long waits.
Learn more about why you should consider clinical risk alongside time-based risk when booking patients.
Chronological Management
Where possible, surgery should be offered to patients in chronological order — in other words, the order in which they arrived on the waiting list.
This can be difficult, as different doctors have different skill sets and different availability. In addition to this, there are legitimate reasons why you might book out of turn, including:
- Session capacity – There is session capacity available that requires a short procedure, a day case procedure, or a type of procedure (e.g cataract LA list, flexi list), so we will bring the appropriate case forward to make the most of theatre time,
- Varied urgency within categories – Urgency categories are too broad and some patients need to be seen sooner than the maximum clinically recommended treat by date
- Patient requirements – Sometimes, a patient’s pre-anesthesia status (ASA rating 1, 2 or 3) may mean they are unable to be seen at a particular facility or on a regular list, so instead, they may need to wait for the right list to become available
But generally speaking, if two people with the same presenting complaint are waiting for the same doctor, require the same procedure, and have similar risk factors… the person who was added to the waiting list first should be seen first.
| Using the SystemView Booked in Turn and Treated in Turn components can make it easier to evaluate if patients are being managed chronologically. |
Book Patients in Turn
Often when dealing with large volumes of patients, booking errors happen. In some cases, bookings may be assigned to those who have not waited long — ahead of those that have waited longer. The consequence of this is that when demand and capacity is very tight, we unnecessarily create long waits (or we make people wait too long).
Reviewing who has been booked in turn allows you to see those patients who are booked vs those who are still awaiting a date and understand if the booking practices are reasonable — and if necessary, change any booking errors being made. This is a proactive way to improve booking practices. The goal is to make fewer unreasonable bookings out of turn and prevent unnecessary long waits, as rescheduling surgery can be unsettling for patients.
Inside SystemView, you’ll find useful charts under these components:
Surgery > Chronological Management > Treated in Turn
Surgery > Chronological Management > Booked in Turn
Retrospectively Review Patients Treated Out of Turn
If you cannot prevent patients from being booked out of turn, retrospectively reviewing those patients who were treated out of turn can give you valuable insights into why these are occurring. These insights can include how many day cases are being brought forward to fill day surgery lists, as well as how many small procedures are being brought forward to fill short blocks of time at the end of theatre lists.
It can be tricky (if not impossible) to use theatre source system reports to see who was treated in and out of turn. That’s where an analytics system like SystemView comes in — joining waitlist data and source system activity data.
In SystemView, the Treated in Turn component looks at the patients that have been operated on vs those that are still waiting for their operation. It generates a list of patients who were on the waiting list and sorts them into order based on their category, doctor, and due date. Then it assesses them against the order they were seen (or not seen) to let you know who was treated in turn and who wasn't.
Improve (Meaningful) Theatre Utilisation
Better utilisation of operating theatres can enable you to schedule more surgeries into a day — which is essential to clearing long wait backlogs. It all comes down to minimising the time each theatre is not occupied by a patient.
80% theatre utilisation (time spent on patients) is generally considered an acceptable benchmark because even the most efficient theatre processes have some lost time for changeovers. However, ways to improve meaningful utilisation include:
- Starting the session on time
- Starting each case on time
- Reducing the length of time of changeover
- Reducing early finishes (in other words, booking in enough and the right patients to fill the entire time)
- Reducing late finishes (as this can lead to other delays)
- Introducing strategies to reduce avoidable day of surgery cancellations
- Having patients on standby
This can make a real difference to waitlists by simply fitting a few extra surgeries in per week.
Theatre productivity is of significant interest to hospital executives and departments of health as theatres are very expensive to run. You can find a lot of articles and resources on ‘the productive theatre’. We particularly like these:
- The Productive Operating Theatre (Clinical Excellence QLD)
- Operating Theatre Efficiency Guideline (Queensland Health)
- Introducing The Productive Operating Theatre Programme in Urology Theatre Suites
Plus, you can read more in our blog on Theatre Utilisation Strategies.
Redistribute Patients Or Lists
In some cases, you may be able to redistribute patients (where clinically appropriate) to another theatre list where there is appropriate time available. For example, if someone is referred to a hospital because they’re experiencing carpal tunnel but the wait times for plastic surgeons are unacceptable, you might be able to refer them to an available orthopaedic surgeon or neurosurgeon instead.
Likewise, if there are some short term demand and capacity imbalances coming up within a speciality, there might be an opportunity for a list or two to be taken from a surgeon who has no immediate patients due and given to a surgeon who needs a little more time.
To be able to successfully do this, teams need to be able to see their demand calculated in time alongside their available operating time. This is not something that can be derived from the waitlist alone. It requires both the count of patients due (waitlist) as well as the expected operating time for each patient. SystemView gives teams the ability to see these insights, as it calculates each performing surgeon’s expected operating time for each procedure.
Pool Waitlists
Rather than assigning patients to individual surgeons or hospitals, you could instead create pooled waitlists for a larger area (jurisdictions or states). This system means that patients can access more resources as they’re available, and it can give providers more flexibility to utilise their resources.
This approach is largely supported by surgeons for some specific cases that are typically routine and not complicated (for example a tonsillectomy, flexible cystoscopy, or colonoscopy) and for patients that are low risk. It does, however, limit ‘continuity of care’. Any pooled waitlists should be designed in a way that manages the risk associated with the loss of continuity of care. For example, you might have guidelines about the types of patients who can go onto the list, communications pathways, and other strategies.
Account for Holidays
Holidays can impact both demand and capacity in surgery. An increase in staff leave often means a reduction in elective operating theatres and surgical beds open. Depending on the location, holiday periods can also mean a change to the emergency board demand.
It’s a good idea to plan for holiday periods. Look ahead at patients who are due during the holiday period and attempt to bring them forward and treat them prior to holidays. Waitlist coordinators can use waitlist projections to see when patients are due and when doctors are taking leave to plan for any known holiday periods. In SystemView, you’ll find the following components:
Surgery > Waitlist > Risks and Projections by Specialty
Surgery > Waitlist > Risks and Projections by Doctor
Allocate Theatres for Emergency
All hospitals that have an operating theatre have an emergency theatre for those patients most in need. These theatres are used to stabilise trauma, perform simple (but urgent) general surgery, stabilise neck of femur fractures, and support women delivering babies via an emergency procedure.
In bigger hospitals with more clinical specialties, there are additional emergency theatres to support a broader range of emergency cases (e.g. orthopaedic trauma).
Due to the urgency of the cases, it can be difficult to understand how much time is needed or routinely distributed to minimise disruption to the elective list.
Looking at a breakdown of how much elective surgery operating time is being used by emergency cases can help you understand how much emergency time is required. Review trends over time to understand if and how demand is changing over time, and whether you need to adjust your resource allocation.
Outsourcing
Outsourcing involves transferring a patient who is on a public hospital waitlist to receive care at a private hospital. However, the cost is paid for by the public hospital, without the patient needing private healthcare.
This strategy is regularly used by public hospitals when there is more demand than they have the capacity to provide. Outsourcing may be required when there has been considerable growth in demand for surgery (short or long term) or when the hospital is at capacity due to unplanned patients that are limiting the number of beds available for surgical patients (for example, during COVID outbreaks).
Outsourcing programmes are run differently across different jurisdictions. Some jurisdictions have pre-negotiated contracts that have been set up by funding commissioners (for example, Surgery Connect in Queensland). Others leave it up to the hospitals themselves to decide what they will offer internally and what they will deliver through a clinical sub-contracting model.
To start the process, patients are often identified by the procedure they are waiting for, reviewed for any clinical risk, contacted by the public hospital, and given the option to be treated at a private hospital. If the patient accepts, they are handed over to the private providers and their administration, and their surgical procedure is provided off-site. Where possible, surgeons prefer that the patient is seen by the same surgeon who recommended the surgical treatment plan in order to maintain continuity of care. Often, this can occur in jurisdictions where doctors work both publicly and privately.
In order to ensure the patient is treated, an outsourced patient is kept on the waitlist until they receive confirmation the patient has been treated. Patients are often ‘suspended’ or made ‘not ready for care’ on the public hospital waiting list until they are notified, so that they are not given multiple booking options.
Health services will find it very useful if they can record and track the demand for patients being treated through outsourcing models. Plus, how much surgical capacity is being used. This can inform demand and capacity insights for future contracts.
Insourcing
Insourcing is when a hospital subcontracts surgical services and procedures that are delivered within the public hospital. This is distinct from locum supply, as the end-to-end service — including bookings, pre-admission assessments, and equipment such as prosthetics supply — is all taken care of. Typically, a patient that is identified for outsourcing may instead be transferred to insourcing. The public hospital is then notified when the surgery is complete so they can remove them from the waiting list.
This approach is often used when public hospitals have theatres available, but are unable to staff them. In long wait resolution strategies, insourcing is often used in theatres after hours (lists run from 5:00pm-9:00pm) and over weekends.
This is a relatively new approach to managing waitlists, but is becoming more and more common.
Remote Monitoring and Telehealth
Following COVID, we’ve seen an increase in telehealth and using technology for remote monitoring and healthcare. These can be used post-surgery by:
- Discharging patients early to virtual wards
- Enabling at-home recovery
- Avoiding readmission
This approach can free up hospital beds as well as clinician time, which means more capacity for surgery.
For example, if a patient has a health condition and knows that they’re getting a chest infection, they can initiate a number of steps without going into the hospital to see a respiratory physician. They could visit their GP, get antibiotics, set up remote monitoring, and start getting better before they need further intervention.
GP Shared Care
In some cases, trained GPs can manage and monitor health conditions with the support of specialised clinicians. Post-surgery shared care with GPs can support early discharge and keep people out of hospitals (and hospital beds), while freeing up clinician time.
Prehabilitation Programs
Prehabilitation is where the patient receives care prior to surgery to improve their function, capability, and fitness so they are less likely to experience postoperative complications and more likely to achieve a better surgical outcome.
Prehabilitation programs are usually led by allied health teams including physiotherapists, occupational therapists, and dieticians. They involve things like exercise programs, environmental assessments, and healthy eating plans to support the patients to achieve their best health, as well as setting up a suitable home environment for them post-discharge.
Less complications, better surgical outcomes, and a safe home to return to usually mean significantly fewer changes or delays to hospital discharge and shorter hospital length of stays. In turn, this means more people can be seen from the waiting list.
Pre-Surgery Communication
Good patient communication can help reduce patient cancellations by ensuring that more patients understand the procedure, what they need to do to prepare (fasting, bowel prep, what to bring to hospital), and the admissions process.
For example, giving them a call the day before to confirm that they’re fit for surgery, are following appropriate fasting measures, and know when to arrive and where to go for their admissions. Or having a mobile application that has resources and sends notifications at different intervals.
Other ways to help hospitals more effectively reach patients with a variety of needs include increasing communication frequency, tailoring the message, offering a range of styles and channels, and using interpreters where needed.
Understand COVID’s Impact
Finally, COVID is an important consideration when developing a waitlist management strategy. This is because it is likely that COVID has created a backlog of long waits. And outsource outside of the additional resources required for managing your COVID-related backlog, your demand and capacity may actually be in balance.
So, what is normal anymore?
It is really hard to know what a normal situation looks like and how treatment delays will impact patients. When elective surgery has been delayed for months or (in some areas) up to three years, what might the future look like? We could see:
- Patients whose condition has deteriorated so much that they are no longer suited to the intended surgery
- Additional health problems that have emerged over time that will impact the intended treatment plan
- Patients who no longer require their surgery as they have passed away or received emergency care for their condition
- Sicker patients when they arrive in clinic as they have delayed their initial referral in order to avoid COVID exposure
- People seeking other treatment options due to long wait times or different expectations of the hospital system
- We just don’t know the long-term impacts yet, but one thing is certain: there are flow-on effects from delaying elective surgery.
If you’re feeling overwhelmed at the task of managing your surgery waitlists — or even just reporting on what your numbers are — hospital improvement software like SystemView could be the answer.
SystemView makes it easier to identify areas of concern and understand the big picture of what’s going on in your hospital, while enabling you to dive into individual domains and specialties.
It makes it possible (in just a few clicks) to see all your resources and how effectively you’re utilising them, with real-time data, trends, and future predictions. You can also see your waitlists so you can check who’s booked in for surgery and identify who you should book next to avoid patients waiting too long.
In fact, everything inside SystemView was originally built around the issue of managing overdue patients in surgery and waiting lists are still one of our most used components today.
| SystemView makes it possible (in just a few clicks) to see all your resources and how effectively you’re utilising them. It makes it easy to identify who you should book next to avoid long waits. |
Some of the key areas and components inside SystemView that can help you manage surgical waitlists include:
| Waiting List | Risks & Projections Trends Procedure Analysis Patient List Operating Times Dynamics End of Next Month End of Current Month |
| Demand & Capacity | Emergency Session Allocation Trends |
| Chronological Management | Treated in Turn Booked in Turn |
| Activity Trends | Elective by Category |
| Theatre Effectiveness | Utilisation Late Starts Late Finishes Knife To Skin Early Finishes Day of Surgery (DOS) Cancellations |
| Emergencies Now | |
| Elective Schedule Monitor |
Feeling overwhelmed? It’s not just you. Hospital executives, department managers, clinicians, and bookings officers in hospitals all over the world are struggling with this issue.
Fixing surgery waitlists could be one of the biggest challenges you tackle in your career.
| Fixing surgery waitlists could be one of the biggest challenges you tackle in your career. |
There are no overnight fixes and it’s a big, multi-faceted problem. But if you can understand the real issues at play, you can create a plan and strategy that'll help you find short-term efficiencies and make a case for long-term change.
The best thing you can do is start today. Begin by looking at your data and uncovering the root causes behind long waits for surgery, then start exploring strategies for those specific problems.
Hospital jurisdictions all over the world are grappling with the same issues relating to surgery waitlist management, and the never-ending balancing act between demand and capacity.
If you learn something interesting from your data analytics or a surgical waitlist management strategy, then share it with others. And if you’re facing a specific issue, reach out for help from the community. Someone else may already have the answer you’re looking for.
Subscribe to our newsletter
Stay up to date with our latest news, tips and blog posts.